Erythropoietin (EPO) is a glycoprotein hormone, naturally produced by the peritubular cells of the kidney, that stimulates red blood cell production. Renal cortex peritubular cells produce most EPO in the human body. PO2 directly regulates EPO production. The lower the pO2, the greater the production of EPO.
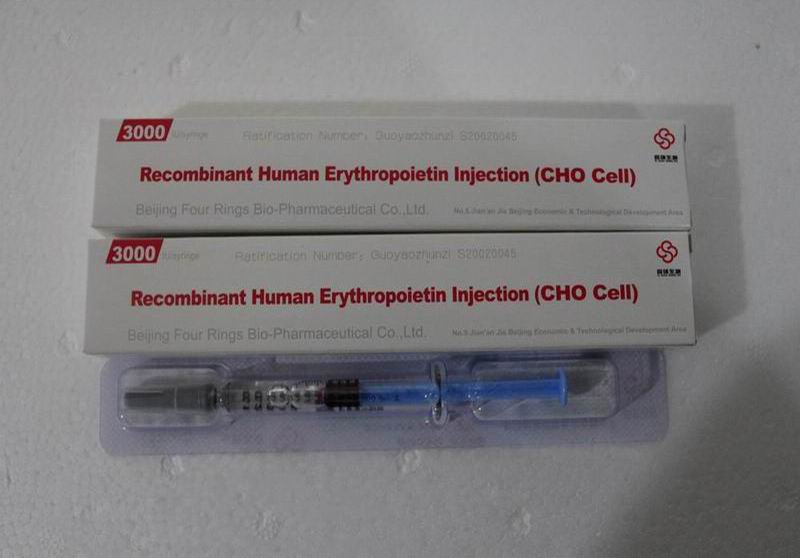
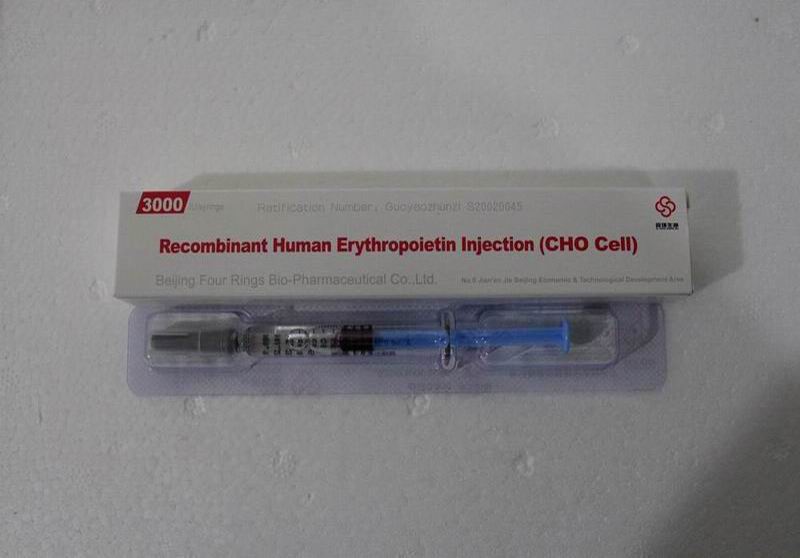


Erythropoietin EPO
- Manufactured by: HygHGH Biopharm Co., Ltd.
- Country of origin: China
- Manufactured since: 2009 – Present
- Package :3000iu/10box/1kits
- Price: $1.5 – $3 per IU
- Minimum Order:1 kits
- Storage:2–8 ℃ in (room temperature)
- Delivery: 5-15 days
- Source: tophygetropin.com/shop/
Erythropoietin stimulating agents (ESAs) are recombinant versions of EPO produced pharmacologically. Examples of ESAs are epoetin, darbepoetin, and methoxy polyethylene glycol-epoetin beta. ESAs are generally indicated in conditions where there is impaired red blood cell production. This activity will highlight the mechanism of action, adverse event profile, pharmacology, monitoring, and relevant interactions of ESAs in light of the natural physiology of erythropoietin, pertinent for members of the interprofessional team in the treatment of patients with conditions where these agents are indicated.
The kidney cells that make erythropoietin are sensitive to low oxygen levels in the blood that travels through the kidney. These cells make and release erythropoietin when the oxygen level is too low. A low oxygen level may indicate a diminished number of red blood cells (anemia), or hemoglobin molecules that carry oxygen through the body.
Erythropoietin (EPO) Indications (benefit & effect)
Erythropoietin (EPO) is a glycoprotein hormone, naturally produced by the peritubular cells of the kidney, that stimulates red blood cell production. Renal cortex peritubular cells produce most EPO in the human body, though in a fetus, the liver is the primary site of production.[1] EPO production also occurs in the spleen, liver, bone marrow, lung, and brain in small quantities. PO2 directly regulates EPO production. The lower the pO2, the greater the production of EPO. Indirectly, low hemoglobin levels stimulate EPO production.
Erythropoietin Stimulating Agents (ESAs) are recombinant versions of EPO produced pharmacologically. Examples of ESAs are epoetin, darbepoetin, and methoxy polyethylene glycol-epoetin beta.
ESAs are generally indicated in conditions where there is impaired red blood cell production. The two primary FDA approved indications for ESAs are anemia secondary to chronic kidney disease and chemotherapy-induced anemia in patients with cancer.Other approved indications are anemia secondary to zidovudine treatment in HIV infection, support in patients receiving autologous blood transfusions, anemic patients undergoing elective surgery (both pre-op and post-op) anemia in preterm infants.
In CKD, where there is damage to the kidneys and limited EPO production by the peritubular cells, ESAs are beneficial. In CKD, ESAs are useful in patients who are receiving dialysis as well as patients soon to need dialysis. The FDA approved the use of epoetin (1993) and darbepoetin (2002) for patients with chemotherapy-induced anemia. In patients with CKD and chemotherapy-induced anemia, ESAs are generally limited to patients with hemoglobin less than 10g/dL due to the risk of adverse effects.
Erythropoietin (EPO) definition and facts
- Measuring blood levels of erythripoietin, a hormone involved in red blood cell production, can diagnose some medical conditions.
- Measuring blood levels of erythripoietin, a hormone involved in red blood cell production, can diagnose some medical conditions.
- Erythropoietin (EPO) is a hormone produced by the kidney.
- Erythropoietin promotes the formation of red blood cells by the bone marrow.
- The erythropoietin hormone level can be detected and measured in the blood (the EPO test).
- Measurement of the blood erythropoietin level can be used to detect certain medical conditions.
- Erythropoietin can be synthesized and used as a treatment of some forms of anemia.
- Erythropoietin has been misused as a performance-enhancing drug by some athletes.
Erythropoietin (EPO) Side Effects
1. General reaction:
A small number of patients may have headaches, low fever, fatigue, etc. at the beginning of the medication. Individual patients may have myalgia and joint pain.
Most of the adverse reactions can be improved after symptomatic treatment, and will not affect the continued use of the drug. In some cases, the above symptoms persist and should be considered for withdrawal.
2. Allergic reactions:
Very few patients may develop allergic reactions such as rash or urticaria after medication, including anaphylactic shock.
Therefore, when using this product for the first time or when using this product again,
It is recommended to use a small amount first, and then confirm that there is no abnormal reaction, and then inject the whole amount.
If abnormalities are found, stop the drug immediately and dispose of it properly.
3. Cardiovascular system:
High blood pressure,
The original hypertension is worsening and there are headaches, disturbances of consciousness, and spasms due to hypertensive encephalopathy.
It can even cause cerebral hemorrhage.
Therefore, attention should be paid to the changes in blood pressure during the treatment of erythropoietin injection.
If necessary, reduce or discontinue the drug and adjust the dose of antihypertensive drugs.
4. Blood system:
As the hematocrit increases, the blood viscosity can be significantly increased.
Therefore, care should be taken to prevent thrombosis.
5. Liver: Occasionally, GOT and GPT rise.
6. Gastrointestinal: Sometimes nausea, vomiting, loss of appetite, diarrhea, etc. occur.
Dosage
1. Renal anemia:
This product should be used under the guidance of a doctor. It can be administered subcutaneously or intravenously, 2 to 3 times a week.
The dose to be administered is adjusted according to the patient’s degree of anemia, age and other relevant factors.
Treatment period: 100 to 150 IU/kg per week for recommended hemodialysis patients and 75 to 100 IU/kg for non-dialysis patients.
If the hematocrit increases by less than 0.5 vol% per week, the dose may be increased by 15 to 30 IU/kg after 4 weeks, but the maximum dose may not exceed 30 IU/kg/week.
Hematocrit should be increased to 30 to 33 vol%, but should not exceed 36 vol% (34 vol%).
Maintenance period:
If the hematocrit reaches 30 to 33 vol% or / and hemoglobin reaches 100 to 110 g / liter, it enters the maintenance treatment phase.
It is recommended to adjust the dose to 2/3 of the therapeutic dose and then check the hematocrit every 2 to 4 weeks to adjust the dose to avoid erythropoiesis, maintain hematocrit and hemoglobin at appropriate levels.
2. Surgical perioperative red blood cell mobilization:
- Applicable to elective surgical patients with preoperative hemoglobin at 100-130 g/l (except for cardiac vascular surgery),
- The dosage is 150 IU/kg, 3 times a week.
- Subcutaneous injection, applied from 10 days before surgery to 4 days after surgery,
- Can reduce intraoperative and postoperative anemia,
- Reduce the need for allogeneic blood transfusions,
- Accelerate the recovery of postoperative anemia.
In order to prevent iron deficiency, the iron can be supplemented at the same time.
Drug contraindications
1. Uncontrolled patients with severe hypertension.
2. Those who are allergic to this product and other mammalian cell derivatives, allergic to human serum albumin.
3. Infected patients, should control the infection and then use this product.
Precautions
1. During the administration of this product, the hematocrit should be checked regularly (once every week, once every two weeks), to avoid excessive erythropoiesis (confirmation of hematocrit below 36 vol%), if excessive Red blood cell growth should be treated appropriately with a pause in medication.
2. The application of this product may cause mild elevation of serum potassium. The diet should be adjusted appropriately. If the blood potassium level rises, the dosage should be adjusted according to the doctor’s advice.
3. For patients with myocardial infarction, pulmonary infarction, cerebral infarction, patients with a history of drug allergy and patients with allergic tendency should be carefully administered.
4. The demand for iron increased due to effective hematopoiesis during treatment.
A drop in serum iron concentration usually occurs. If the patient’s serum ferritin is below 100 ng/ml, or if the transferrin saturation is less than 20%, iron should be replenished daily.
5. Folic acid or vitamin B12 deficiency will reduce the efficacy of this product. Excessive aluminum can also affect the efficacy.
Questions to ask your doctor
Diagnosis of problems with erythropoietin is often done through blood tests that measure red blood cell counts. If you are concerned about your red blood cell count, talk to your doctor. You may wish to ask:
- Could erythropoietin be the source of my blood cell count problems?
- What treatments are available?
- What lifestyle changes could I make to help?
- What underlying conditions could be causing this problem?
- If you do not have an endocrinologist, you need to find a qualified one to help you with these questions. Use our effective directory to find an endocrinologist in your area, and get started on learning more about your hormone health.
Storage Of Goldtropin Hgh
Storage:2–8 ℃ in room temperature
Erythropoietin (EPO) Mixed reviews Summary
Erythropoietin (EPO) primarily activates erythroid cell proliferation and growth and is active in several types of non-hematopoietic cells via its interaction with the EPO-receptor (EPO-R). This review focuses on the role of EPO in skeletal muscle. The EPO-R is expressed in skeletal muscle cells and EPO may promote myoblast differentiation and survival via the activation of the same signaling cascades as in hematopoietic cells, such as STAT5, MAPK and Akt. Inconsistent results exist with respect to the detection of the EPO-R mRNA and protein in muscle cells, tissue and across species and the use of non-specific EPO-R antibodies contributes to this problem. Additionally, the inability to reproducibly detect an activation of the known EPO-induced signaling pathways in skeletal muscle questions the functionality of the EPO-R in muscle in vivo. These equivocal findings make it difficult to distinguish between a direct effect of EPO on skeletal muscle, via the activation of its receptor, and an indirect effect resulting from a better oxygen supply to the muscle. Consequently, the precise role of EPO in skeletal muscle and its regulatory mechanism/s remain to be elucidated. Further studies are required to comprehensively establish the importance of EPO and its function in skeletal muscle health.
Erythropoietin (EPO) review
- Availability
- Reputability
- Purity
- Price
- Cost Effectiveness